When your pancreas swells up, it doesn’t just hurt-it disrupts everything. Digestion, blood sugar, energy levels, even your ability to eat without pain. Pancreatitis isn’t one condition. It’s two very different diseases with the same name: acute and chronic. One comes on fast, often after a night of heavy drinking or a gallstone. The other creeps in slowly, silently, and changes your life forever. And no matter which one you’re dealing with, nutrition isn’t just advice-it’s part of the treatment.
What Happens When Your Pancreas Gets Inflamed?
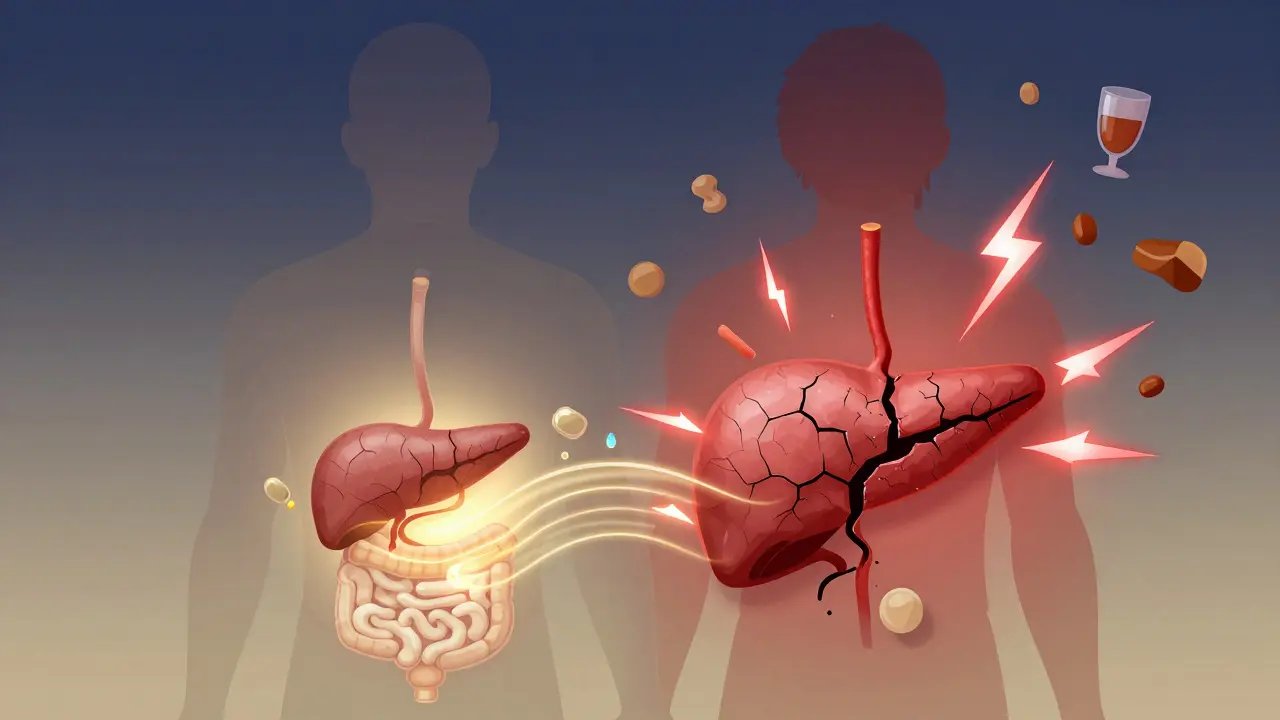
Your pancreas is a quiet worker. It sits behind your stomach, making enzymes to break down food and insulin to control blood sugar. In acute pancreatitis, those enzymes turn on too early-inside the pancreas itself-and start digesting the organ from the inside out. That’s why the pain hits like a brick: sharp, constant, radiating from your upper belly to your back. You might feel nauseous, vomit, or get a fever. Most people get better in a few days with fluids, rest, and pain control. About 80% recover fully. But in chronic pancreatitis, the damage doesn’t heal. Repeated inflammation turns healthy tissue into scar tissue. The pancreas slowly loses its ability to make enzymes and insulin. Pain becomes a constant companion, often worse after eating. Weight loss isn’t from lack of appetite-it’s from malabsorption. Your body can’t break down fats, proteins, or vitamins. Fatty, foul-smelling stools (steatorrhea) become normal. Diabetes can develop. And the risk of pancreatic cancer rises.Acute vs. Chronic: The Key Differences
It’s easy to confuse the two. But they’re not the same disease. Here’s how they really differ:- Onset: Acute hits suddenly. Chronic builds over years.
- Pain: Acute pain is intense and constant. Chronic pain is often post-meal, dull, and may even fade over time as the pancreas wears out.
- Recovery: Acute can fully resolve. Chronic never does-it only gets worse without intervention.
- Lab tests: Acute shows sky-high lipase and amylase. Chronic may show normal enzyme levels because the pancreas has nothing left to produce.
- Imaging: Acute shows swelling. Chronic shows calcifications, duct changes, or shrinkage.
Why Nutrition Is Non-Negotiable in Recovery
You can’t out-drug bad nutrition. In acute pancreatitis, the goal is to let the pancreas rest. That means no food at first-just IV fluids. But that doesn’t mean starving. Research shows starting enteral feeding (through a tube into the small intestine) within 24 to 48 hours cuts infection risk by 30%. Delaying nutrition doesn’t help. It hurts. For chronic pancreatitis, nutrition becomes lifelong management. You’re not just eating to feel full-you’re eating to survive.- Enzyme replacement is essential. Without it, you can’t absorb fats, proteins, or fat-soluble vitamins (A, D, E, K). Dosing matters: 40,000-90,000 lipase units per main meal, 25,000 per snack. Too little? You keep losing weight. Too much? You get abdominal cramping.
- Fat restriction isn’t always the answer. In the acute phase, you might need under 30 grams of fat per day. But in chronic, you don’t need to avoid fat entirely-you need the right kind. Medium-chain triglycerides (MCTs), found in coconut oil or specialized supplements, bypass the need for pancreatic enzymes. They’re absorbed directly into the bloodstream.
- Small, frequent meals. Six to eight small meals a day reduce the burden on your pancreas and help stabilize blood sugar. Large meals trigger more pain and worse malabsorption.
- Supplement deficiencies. Studies show 85% of chronic pancreatitis patients are low in vitamin D. 40% lack B12. 25% are deficient in vitamin A. These aren’t optional. You need daily supplements, often in high doses.

What Not to Do
Some advice you hear is dangerous.- Don’t stop enzymes because you feel better. The pancreas doesn’t magically recover. Stopping enzymes means your body stops absorbing nutrients. Weight loss returns.
- Don’t rely on over-the-counter supplements. Most don’t contain enough lipase. Prescription enzymes like Creon or Pancreaze are formulated to survive stomach acid and activate in the right place.
- Don’t ignore smoking. Quitting smoking is the single most effective way to slow chronic pancreatitis progression. Smokers have twice the rate of disease worsening compared to those who quit.
- Don’t avoid protein. You need 1-1.5 grams of protein per kilogram of body weight daily. Muscle loss is common-and deadly.
The Hidden Complications
Pancreatitis doesn’t just hurt. It changes your body long-term.- Diabetes: Called pancreatogenic or type 3c diabetes, it’s different from type 1 or 2. Blood sugar swings wildly because the pancreas can’t release insulin properly. Continuous glucose monitors (like Dexcom G7, approved in 2024) help track these unpredictable spikes and drops.
- Pain management: Opioids are often prescribed, but 30% of chronic pancreatitis patients develop opioid use disorder within five years. Non-opioid options-nerve blocks, acupuncture, cognitive behavioral therapy-are increasingly part of care.
- Cancer risk: Chronic pancreatitis increases pancreatic cancer risk by 15 to 20 times. While most won’t get it, annual MRI or MRCP scans are recommended for high-risk patients, especially those with genetic mutations or long-standing disease.
- Malnutrition: Losing 10% of your body weight is common. Some patients end up on feeding tubes. A 2023 study found that 42% of patients lost over 10% of their weight because they feared eating would trigger pain.
What’s New in Treatment
The field is evolving.- New enzyme formulations: Creon 36,000 improved fat absorption by 45% compared to older versions. Non-porcine enzymes (like Liprotamase) are in trials for people allergic to pig-derived products.
- Stem cell therapy: The REGENERATE-CP trial is testing whether stem cells can repair damaged pancreatic tissue. Early results show 30% improvement in enzyme production after one year.
- Probiotics: Lactobacillus rhamnosus GG and Bifidobacterium lactis reduced pain scores by 40% in a 2023 gut microbiome study.
- Biomarkers: Pancreatic stone protein (PSP) can now predict severe acute pancreatitis within 24 hours, helping doctors decide who needs aggressive care.
How to Get the Right Care
Finding a specialist matters. A 2023 survey found that 60% of patients struggled to find a doctor who understood pancreatitis. Average wait time to see a pancreatic expert? Over four months. Look for centers with multidisciplinary teams: gastroenterologists, dietitians, pain specialists, endocrinologists. These aren’t luxury add-ons-they’re essential. If you’re managing this yourself, keep a food and symptom journal. Track meals, enzyme doses, pain levels, stool frequency, and weight. Bring it to every appointment. Most doctors don’t have time to dig into your history-your notes do the work for you.Final Thought: This Is a Lifelong Journey
Acute pancreatitis is a wake-up call. Chronic pancreatitis is a lifestyle overhaul. Both demand respect. You can’t cure it, but you can control it. Eat the right way. Take your enzymes. Quit smoking. Avoid alcohol. Monitor your blood sugar. Supplement what’s missing. See the right specialists. The goal isn’t perfection. It’s stability. It’s being able to sit at the table with your family without fear. It’s gaining back the weight you lost. It’s sleeping through the night. Your pancreas can’t heal. But with the right care, you can still live well.Can you recover from chronic pancreatitis?
No, chronic pancreatitis causes permanent damage. Scar tissue replaces healthy cells, and the pancreas can’t regenerate. But with proper treatment-enzyme replacement, diet changes, quitting smoking, and managing pain-you can slow progression, prevent complications, and live a full life. Recovery isn’t about healing the organ. It’s about managing the disease.
What foods should I avoid with pancreatitis?
Avoid fried foods, fatty meats (bacon, sausage, ribs), full-fat dairy, butter, cream, pastries, and alcohol. In acute phases, limit total fat to under 30 grams per day. In chronic stages, focus on low-fat, nutrient-dense foods: lean proteins (chicken, fish, tofu), whole grains, vegetables, fruits, and healthy fats like avocado and olive oil in small amounts. MCT oil is a special exception-it’s absorbed without enzymes.
Do I need to take pancreatic enzymes forever?
If you have chronic pancreatitis and signs of exocrine insufficiency (fatty stools, weight loss, nutrient deficiencies), yes. Enzymes aren’t optional-they replace what your pancreas can no longer make. Skipping them leads to malnutrition, muscle loss, and bone density problems. Dosing should be adjusted based on symptoms and stool fat tests, not how you feel.
Can pancreatitis cause diabetes?
Yes. When the pancreas is damaged, it can’t produce enough insulin. This is called type 3c diabetes. It’s different from type 1 or 2. Blood sugar swings are harder to predict. Many patients need insulin. Continuous glucose monitors (CGMs) are now recommended because standard finger-stick tests often miss dangerous lows and highs.
How do I know if my enzyme dose is right?
Signs your dose is too low: persistent fatty stools, ongoing weight loss, bloating after meals. Your doctor can order a 72-hour fecal fat test to measure how much fat you’re excreting. If it’s above 7%, your dose needs adjustment. Don’t wait for symptoms to worsen-ask for testing if you’re still losing weight or feeling weak.
Is it safe to drink alcohol after having acute pancreatitis?
No. If alcohol caused your acute pancreatitis, continuing to drink raises your risk of developing chronic pancreatitis by up to 90%. Even if your attack wasn’t alcohol-related, drinking increases inflammation and slows healing. Complete abstinence is the only safe choice.
Can nutrition alone reverse pancreatitis damage?
No. Nutrition supports recovery and prevents complications, but it can’t repair scar tissue or restore lost enzyme production. Enzyme replacement, medication, and lifestyle changes are required. Think of nutrition as the foundation-not the cure.
What’s the best way to gain weight with chronic pancreatitis?
Focus on calorie-dense, low-fat, high-protein foods: shakes with MCT oil, Greek yogurt, eggs, lean chicken, nut butters (in moderation), and protein supplements. Eat small meals every 2-3 hours. Work with a dietitian to calculate your daily calorie needs-most patients need 2,500-3,000 calories a day to maintain weight. Weight gain is slow, but possible with consistency.














Lisa Cozad
January 11, 2026 AT 12:05