Chronic heartburn isn’t just annoying-it can change the lining of your esophagus in ways that put you at risk for cancer. If you’ve had acid reflux for more than 10 years, especially if it’s happening several times a week, you might be developing something called Barrett’s esophagus. It doesn’t cause new symptoms. You won’t suddenly feel different. But underneath the surface, your body is changing in a way that needs attention.
What Exactly Is Barrett’s Esophagus?
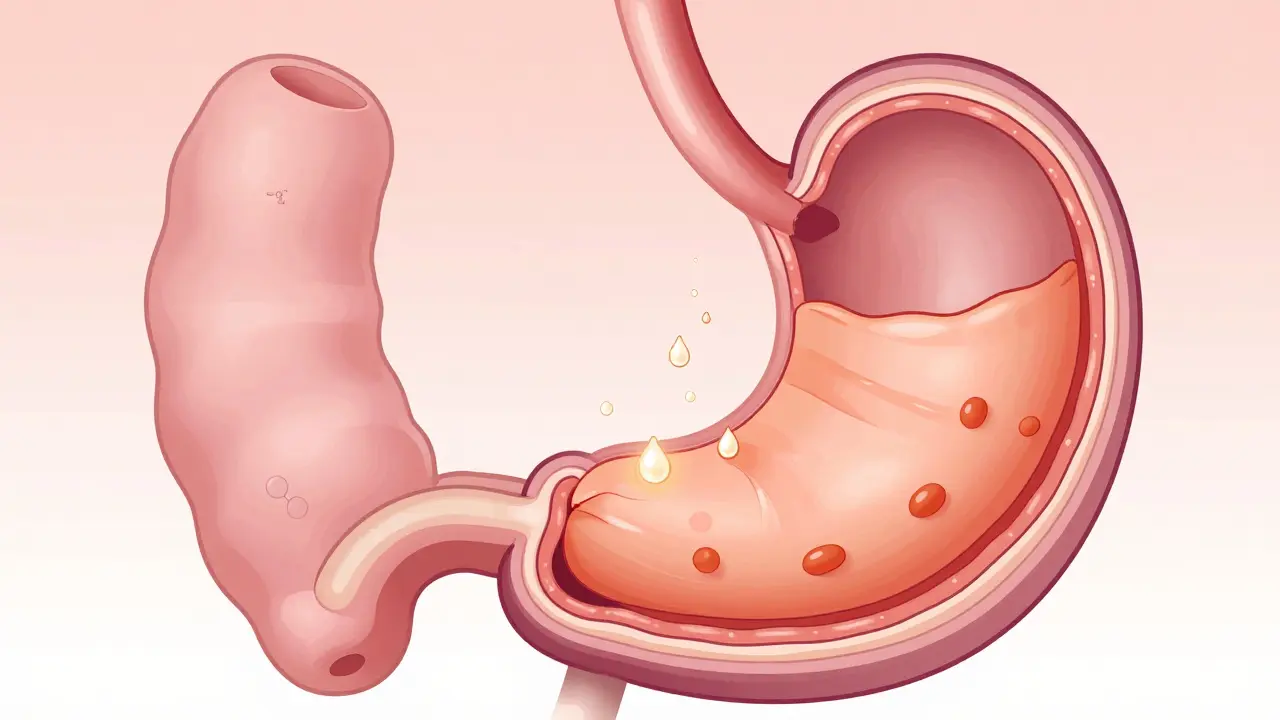
Barrett’s esophagus happens when the normal pink, flat lining of your esophagus-made of squamous cells-gets replaced by a different kind of tissue: columnar cells that look like the lining of your intestine. This is called intestinal metaplasia. It’s not cancer. But it’s a warning sign. This change is your body’s attempt to protect itself from repeated damage by stomach acid. The problem? This new tissue is more likely to turn into cancer over time.
The condition was first described in 1950 by Norman Barrett in London. Today, about 5.6% of the U.S. population has it. Among people with long-term GERD, that number jumps to 10-15%. Men are three times more likely to develop it than women. White men over 50 with a history of smoking or obesity are at the highest risk. The longer you’ve had acid reflux-especially more than three times a week for over 20 years-the higher your chance of developing Barrett’s. In fact, this group has a 40-fold increased risk of esophageal cancer compared to someone without GERD.
Why It’s Dangerous
Barrett’s esophagus doesn’t cause pain, difficulty swallowing, or new symptoms. That’s why it’s so dangerous. People often ignore their heartburn, thinking it’s just indigestion. By the time they see a doctor, the condition may have already progressed. The real danger isn’t Barrett’s itself-it’s what it can turn into: esophageal adenocarcinoma.
Only about 5% of people with Barrett’s will ever develop cancer. But if they do, the survival rate is poor. Less than 20% live beyond five years after diagnosis. That’s because esophageal cancer often spreads before it’s found. The progression usually follows a path: chronic acid damage → metaplasia (Barrett’s) → low-grade dysplasia → high-grade dysplasia → cancer. High-grade dysplasia alone carries a 6-19% chance of becoming cancer each year.
How Is It Diagnosed?
You can’t diagnose Barrett’s esophagus with a blood test or an X-ray. The only way is through an upper endoscopy. During the procedure, a doctor inserts a thin, flexible tube with a camera into your esophagus. They look for a salmon-colored patch of tissue above the junction where the esophagus meets the stomach. Normal tissue is pale and smooth. Barrett’s tissue looks redder and rougher.
But visual inspection isn’t enough. The diagnosis requires biopsies. The standard method is the Seattle protocol: taking four tissue samples every 1-2 centimeters along the abnormal area. That means 12 to 24 biopsies in one session. Why so many? Because dysplasia can be patchy. A single biopsy might miss it.
Biopsies are graded into four categories:
- Non-dysplastic Barrett’s esophagus (NDBE): No abnormal cell changes. Most common.
- Indefinite for dysplasia: The pathologist isn’t sure. Needs repeat testing.
- Low-grade dysplasia (LGD): Early signs of abnormal cells. Still not cancer, but closer.
- High-grade dysplasia (HGD): Severe changes. Nearly cancer. Requires treatment, not just monitoring.

Who Should Be Screened?
Not everyone with heartburn needs an endoscopy. Screening is targeted. The American College of Gastroenterology recommends it for men who have:
- Chronic GERD symptoms (lasting more than 5 years)
- Symptoms occurring at least once a week
- Plus at least one risk factor: age over 50, White race, smoking history, or central obesity (belly fat)
Women and men without these risk factors rarely benefit from routine screening. The cost and risks of endoscopy outweigh the benefit for low-risk groups. Still, if you’ve had symptoms for over 10 years-even if you’re not in the typical risk group-it’s worth discussing with your doctor.
One major issue? Many people go years without diagnosis. The Esophageal Cancer Action Network found that 68% of Barrett’s patients had symptoms for over five years before being tested. Why? Because they thought heartburn was normal. Or their doctor didn’t raise the concern.
What Happens After Diagnosis?
Management depends on the level of dysplasia.
Non-dysplastic Barrett’s (NDBE): You’ll need an endoscopy every 3-5 years. No treatment is needed unless symptoms worsen. Proton pump inhibitors (PPIs) like omeprazole or pantoprazole are still recommended to reduce acid, even though they don’t eliminate cancer risk.
Low-grade dysplasia (LGD): First, a second pathologist should confirm the diagnosis. Then, surveillance every 6-12 months. But here’s the big change: since 2022, the American Gastroenterological Association now recommends treatment for all confirmed LGD, not just monitoring. Radiofrequency ablation (RFA) has become the standard. In trials, RFA eradicated dysplasia in over 90% of cases, with results lasting over five years.
High-grade dysplasia (HGD): This is a red flag. Surveillance isn’t enough. Treatment is urgent. RFA or cryotherapy can remove the abnormal tissue with 90-98% success. Some patients even get their Barrett’s lining completely eliminated. One Mayo Clinic patient reported full recovery after six months of treatment.
Treatment Beyond Endoscopy
Medication alone won’t reverse Barrett’s. But it’s still essential. High-dose PPIs (like omeprazole 40mg twice daily) are standard. Yet studies show even this doesn’t fully stop acid reflux in 30-45% of patients. That’s why doctors now recommend esophageal pH monitoring to check if your medication is truly working-not just whether your heartburn improved.
Lifestyle changes make a huge difference:
- Stop eating 3 hours before bed
- Elevate the head of your bed by 6-8 inches
- Avoid fatty foods, chocolate, caffeine, alcohol, and spicy meals
- Keep your BMI under 25
- Quit smoking
Weight loss alone can reduce reflux episodes by 40%. Even losing 10 pounds helps.
The Future of Screening
Endoscopy is invasive, expensive, and not always accurate. The U.S. spends $1.2 billion a year on Barrett’s screening and surveillance. And yet, 95% of people with Barrett’s will never get cancer. That means most endoscopies are done for no reason.
New tools are emerging. The TissueCypher Barrett’s Esophagus Assay, approved by Medicare in 2021, analyzes biopsies for molecular markers. In a 635-patient study, it had a 96% negative predictive value-meaning if the test says low risk, you almost certainly won’t develop cancer in the next three years. This could cut unnecessary endoscopies by half.
Another promising area? DNA methylation tests. Researchers in Texas are testing blood and tissue markers that could predict who’s likely to progress to cancer. A $2.4 million study running until 2026 aims to identify patterns that signal danger. If successful, we could move from blanket surveillance to personalized risk-based screening.
What You Should Do
If you’ve had daily heartburn for over 10 years, especially if you’re a man over 50 with other risk factors:
- Don’t wait for symptoms to worsen.
- Ask your doctor about an endoscopy.
- If diagnosed with Barrett’s, get biopsies done properly using the Seattle protocol.
- Follow up consistently-don’t skip endoscopies because you feel fine.
- Take PPIs as prescribed and make lifestyle changes.
Barrett’s esophagus is silent. But it doesn’t have to be deadly. Early detection and proper management can prevent cancer before it starts. The goal isn’t to eliminate every case of Barrett’s-it’s to find the few that are heading toward cancer and stop them before it’s too late.
Can Barrett’s esophagus go away on its own?
No, Barrett’s esophagus doesn’t reverse itself without treatment. The abnormal tissue stays unless it’s removed through endoscopic procedures like radiofrequency ablation. Even if your symptoms improve with medication, the tissue change remains. That’s why ongoing surveillance is critical.
Do proton pump inhibitors (PPIs) prevent cancer in Barrett’s esophagus?
PPIs help control acid and reduce inflammation, but they don’t eliminate cancer risk. Studies show that even with perfect symptom control, some patients still develop dysplasia. PPIs are part of management, but they’re not a cure. Complete acid suppression-confirmed by pH testing-is more effective than just treating heartburn.
Is Barrett’s esophagus hereditary?
There’s no single gene for Barrett’s, but family history does matter. People with a first-degree relative (parent, sibling) who had Barrett’s or esophageal cancer have a higher risk. This suggests genetic factors may influence how the body responds to acid damage, though the exact mechanism isn’t fully understood yet.
Can women develop Barrett’s esophagus?
Yes, but it’s much less common. Women make up only about 21% of Barrett’s cases, even though they’re nearly half the population. This is likely because men are more likely to have long-term, severe GERD, higher rates of smoking and obesity, and differences in how acid reflux affects their esophagus. Still, any woman with chronic GERD for over 10 years should discuss screening.
What happens if I skip my surveillance endoscopy?
Missing endoscopies increases your risk of undetected cancer. Dysplasia can develop slowly and without symptoms. A single missed check-up could mean missing the window to treat high-grade dysplasia before it turns into cancer. Studies show patients who don’t follow surveillance guidelines are 3-5 times more likely to be diagnosed with advanced esophageal cancer.
Are there alternatives to endoscopy for screening?
Not yet as reliable, but emerging options exist. The TissueCypher test analyzes biopsy samples for molecular markers and can predict cancer risk with high accuracy. Capsule endoscopy and swallowable balloon devices are being tested, but none have replaced traditional endoscopy yet. For now, endoscopy with biopsy remains the gold standard.















Charity Hanson
February 27, 2026 AT 15:19